Earlier posts on this blog and others have sought to tease out some of the issues that have been brought to light with the Australian government's attempts at reform of maternity care.
Since mid-2008, with the announcement of the
Maternity Services Review, midwives and birthing activists have written and argued and pleaded for improvements that are based on evidence and women's rights.
That campaign is ongoing. There is plenty of work to be done.
Some midwives are now seeking to take up the offer of Medicare (MBS) and limited prescribing rights (PBS) that have progressed through legislation, and are now being implemented.
Each midwife has some serious hurdles that we will need to overcome in order to be granted these 'privileges', and enabling our clients to claim Medicare rebates on services that are linked to Medicare items. Perhaps the most challenging is the requirement, spelt out in the
National Health (Collaborative arrangements for midwives) Determination 2010 for an authorised midwife to have a signed collaborative arrangement with a doctor, or alternatively to follow a lengthy and prescriptive documentation process.
Of the options for signed arrangements, the first option is that the midwife
is employed by the doctor or doctors. This is not a likely option for midwives who practise privately in communities. Obstetric group practices already employ midwives in their rooms, and these midwives probably provide valuable assistance in seeing the large numbers of women who pass through the rooms. But it is doubtful whether, even if these midwives are granted eligibility for MBS and PBS, they will be encouraged by their bosses to practise authentic midwifery, including practising on their own authority, promoting normal birth, and working in partnership with women throughout the episode of care. These midwives are likely to continue as obstetric assistants: some may scrub to assist at caesareans; some may even take on a caseload. But unless they are practising in true co-labor, as professionals in their own right, the 'reforms' are unlikely to make any changes to maternity care standards or outcomes.
The second option for signed arrangements is that the woman is
"referred, in writing, to the midwife for midwifery treatment by a specified medical practitioner". This option is quite fascinating. The obvious question is, why would a "specified medical practitioner" - a doctor who makes a living that is proportionate to the number of women who receive private maternity services from him or her, refer a woman to a midwife? This option will require strong women who approach these doctors, armed with their own plan, and request a referral that meets the requirements for collaborative arrangements.
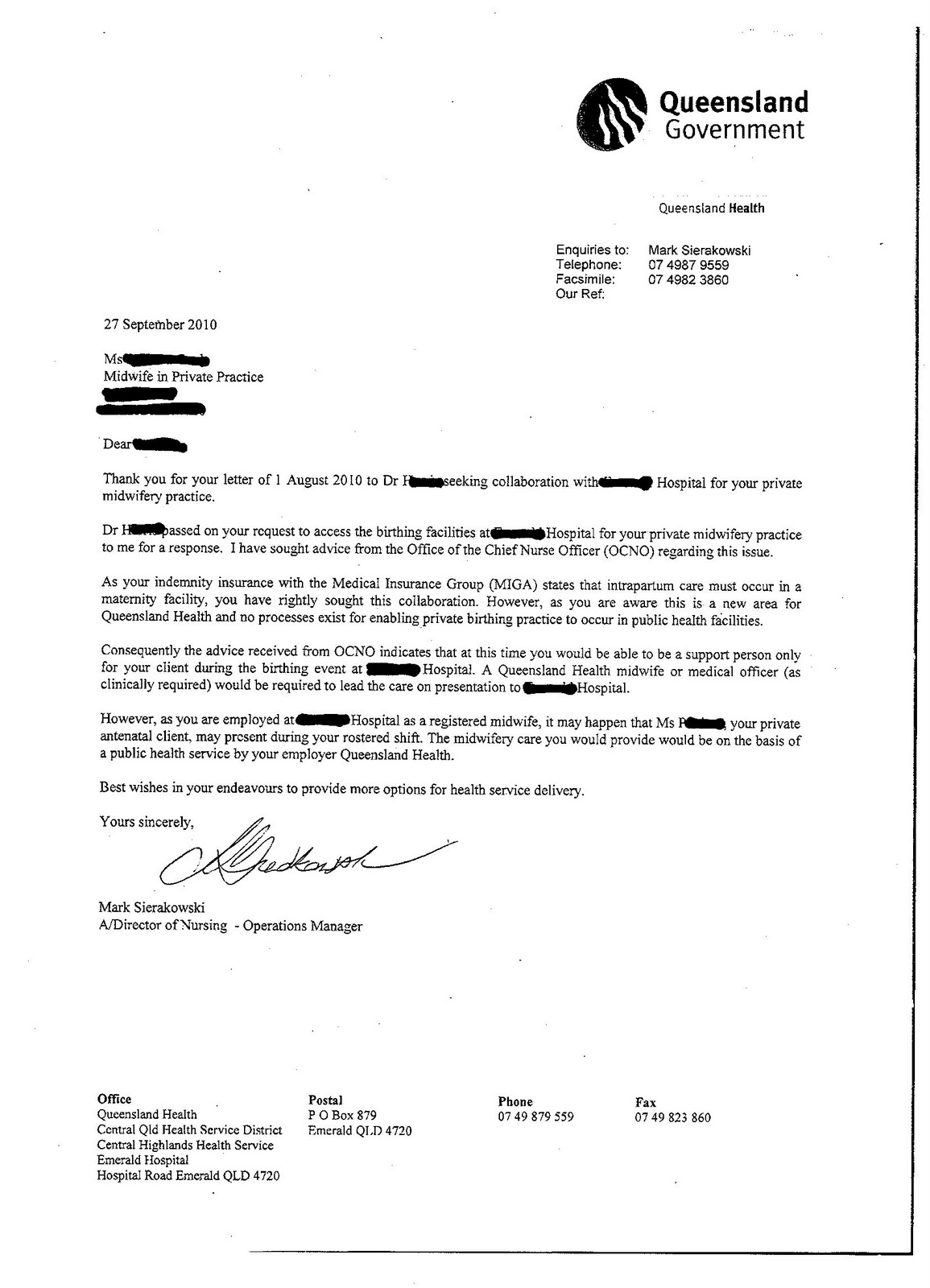
The third option for signed arrangements appears to be the one that may be suitable for midwives who are practising privately and attending home births. This option will require the specified medical practitioner to be
"a medical practitioner employed or engaged by a hospital authority and authorised by the hospital authority to participate in a collaborative arrangement." In this scenario the doctor who signs the arrangement may not be the doctor who provides collaboration in situations when women in our care, who are planning home birth, are referred to the hospital for obstetric review, such as for prenatal assessment or monitoring, or transfer of care. The doctor who signs the agreement with the midwife may be the medical director or head of obstetrics in a public hospital, who delegates the
"authority to participate in collaborative arrangements" to the obsterics registrar. Such collaboration is applicable to the midwife’s provision of private prenatal care, and postnatal care. There is no Medicare item number for intrapartum midwifery care in the community (homebirth), so collaborative arrangements are not required to cover home birth.
Midwives who contact their local public hospitals with the purpose of seeking a signed collaborative arrangement are encouraged to communicate with APMA, or
MIPP, in reporting the responses of the hospitals. These responses will be important information that will be used in reviewing and revising the legislation in the coming year(s).








{kind=link}
{kind=link}
{kind=link}
{kind=link}