{kind=link}
 |
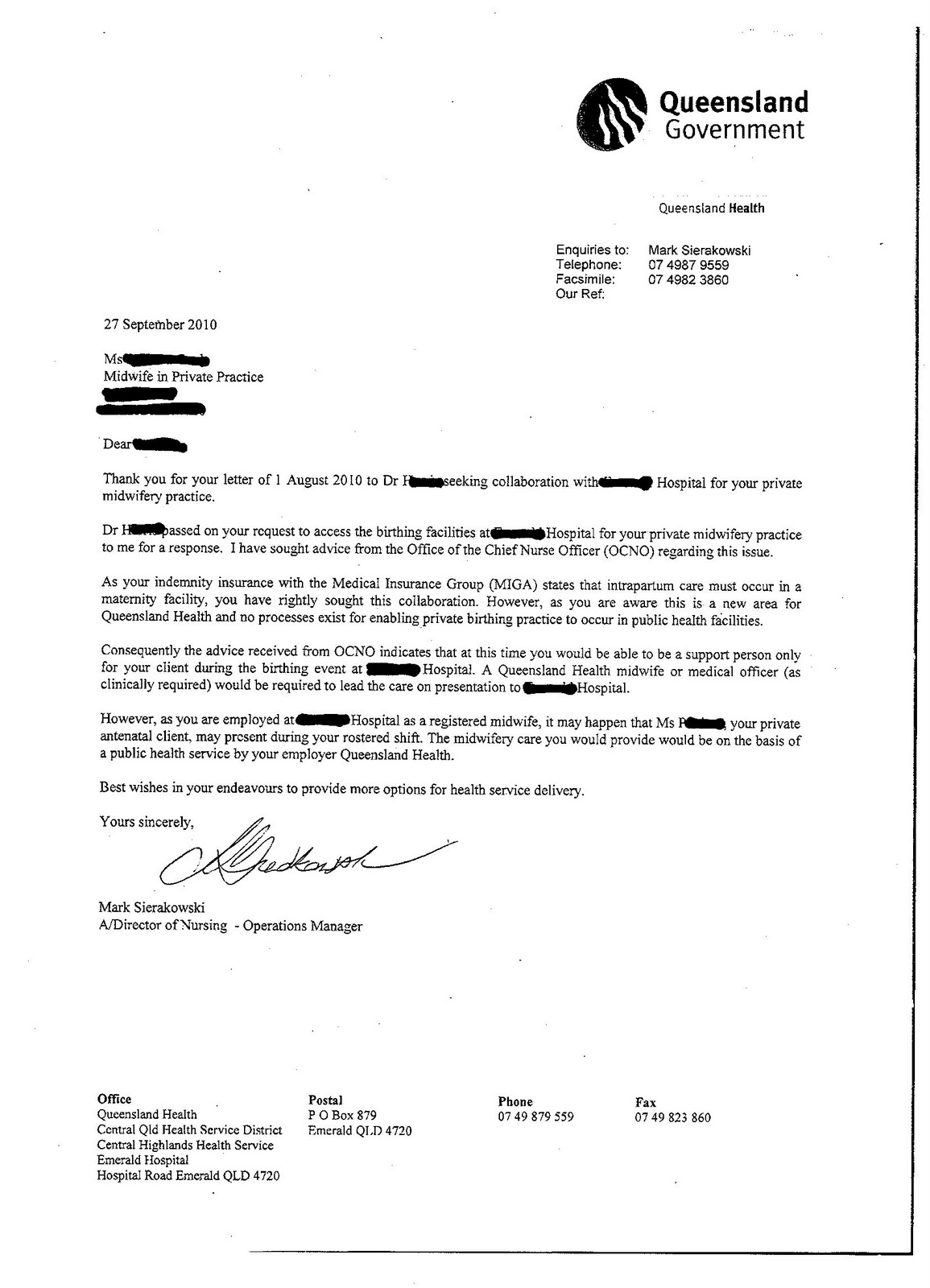
| Letter |
{kind=link}
I have had various discussions with managers/project officers who are attempting to roll out hybrid 'midwifery models of care' for the rural sector. From my own personal observations -
- It is clear that GP's are the primary carer with the midwife as the after thought so as not to upset them.
- GP's are scared they will lose an income stream to their rural practice often with the right to private practice to the local hospital.
- Managers do not want to lose the doctor as the rural community backlash will be fast and vicious (rightly so).
- Higher places of office are providing non-reassuring advice to the facility managers, happy to provide details specific to my application verbally.
- It is clear managers are thinking they can switch a midwife's hat on for a few hours of the day to provide antenatal care or birth care. Essentially they are employed as a nurse first.
- It is clear until nursing workforce shortages are addressed there will be no change in practice in rural areas that ensure continuity of care with a known midwife as midwives 'offering' themselves to be in these new models are still being put on rosters and not annualised salaries plugging up nurse shortages. Burn out for midwives will occur rapidly.
Geographical boundaries in keeping care within local communities to ensure the care is local, owned by the consumer and feels safe (Rebirthing Report) are being ignored in the drive for efficiencies in combining some projects when viewed in a remote office in some districts.