Women’s Right to bodily autonomy and a midwife’s right to practice: We’ll just have to “suck it and see”
Writer: Anonymous
Historic times yet I get the distinct feeling they won’t want to be remembered. Julia Gillard, a declared feminist and yet we are on the cusp of the most draconian midwifery regulation dressed up as reform. From November 1 midwives will be able to claim Medicare funding but only when controlled by a doctor. Midwives are educated and registered to provide complete care for healthy women. Despite common misconception midwives are not handmaidens to doctors, but professionals in their own right.
Naturally it is appropriate for midwives to have established links to a range of other health professionals, this enables a woman to receive timely advice and care. When a midwife and obstetrician are respected for their role and a woman is recognised as the primary decision maker, best practice care is possible. This does not happen in Australia. Many women have been led to believe that their bodies are revolting, faulty with birth a barbaric process that should be managed. Couple this with a system that has financially rewarded huge increases in surgery with little scrutiny, indeed one that saw the likes of Graeme Reeves [NSW the 'Butcher of Bega'] continue to practice. It’s easy to see why obstetrics controls childbirth’s billion-dollar industry.
Maternity reform was the first cab off the health reform rank. Considering it’s the highest volume area, accounting for the greatest number of bed stays, that seemed appropriate to reform advocates. Perhaps this was Minister Roxon’s first mistake, she was overheard saying ‘I want to get maternity over with first and then move onto chronic disease’. I am sure she understood the turf war and passionate consumer advocates it seems she had little understanding of how political (read profitable) pregnant woman are.
Allegedly the AMA threatened a $7 million anti-government campaign pre election if midwives were able to claim Medicare in their own right. Their deal that individual doctors controlled midwives access to funding and the decisions of the birthing woman. If a woman makes a decision not supported by an individual doctor access to funding and midwifery care is likely to be withdrawn.
It is possible that the Gillard Government is contravening its responsibilities under the Convention of the Elimination of all forms of Discrimination Against Women (CEDAW). If international convention is too abstract then perhaps the plight of rural and remote women is more convincing. In rural areas, GP’s control maternity care, even when a GP has ceased obstetric practice the establishment of midwifery models has been vigorously opposed.
Women are forced to relocate or risk travel in labour rather than access local midwifery models. The cultural damage for Aboriginal women is considerable. If Medicare funding was not shackled to the permission of an individual medical practitioner midwives could establish rural clinics. This could have enhanced safety and removed the financial and emotional burden of many rural families.
These and many other issues were formally raised. The Maternity Services Review received 950 submissions, nearly double that of the National Health and Hospitals Reform Commission. The consumer led juggernaut then continued to achieve the nigh impossible, 2 Senate enquires into the same bill (something only seen a handful of times) coupled with a Senate record number of submissions, 2507. Over three thousand gathered outside Parliament House to protest the way the reform in September 2009.
The political cost has been high with Minister Roxon embarrassed by poor advice. It is unclear why but a senior bureaucrat and ministerial adviser both with carriage of maternity reform have both ‘moved on’.
Last week ‘reform representatives’ met with the Minister, the meeting was only achieved after the same women ran in ultra marginal seats in the recent federal election. While seemingly having an open door policy to the AMA, maternity consumers have been repeatedly refused access.
Many criticised the Rudd/Roxon health reform citing it was rather hospital reform, with little focus on health, wellness or consumer engagement. Perhaps that can be explained with yet another medical practitioner appointed by the Minister. Dr Judy Searle, an Obstetrician, seemed unmoved by the participants pleas regarding rural maternity services citing it as ‘a hard area’ but the quote of the meeting must go to the Minister herself who is reported to have responded to the participants comments regarding women’s rights to self determination rather than proposed medical control by saying we will just have to “suck it and see”. So that’s how Labor feminists do women’s rights.
Note: This essay was sent anonymously to APMA.
Wednesday, October 27, 2010
Thursday, October 21, 2010
Disrespect and abuse of women in childbirth
 |
| Rally outside AMA House in Melbourne |
{kind=link}
Many anecdotal accounts are available. Many women and midwives wrote their stories in submissions to the Australian government's Maternity Services Review.
Two well known academics in the field of women's studies have asked that midwives and mothers who are willing to share their stories contact them. This is not, at this stage, funded research. The aim is to make up a collection of accounts that demonstrate issues of women's autonomy and rights in birthing - as both birthgivers and the women workers who care for them. These accounts will be useful in presentations to human rights advocates, and women's health networks.
If you would like your story considered for this project, please send a message to Joy [joy@aitex.com.au].
Click here to read of the US
Thursday, October 14, 2010
WA Health Department statement on Home Birth
Home Births
In Australia there are a small number of women who elect to have home births. In WA, approximately 200 women have a homebirth each year representing between 0.65-0.8% of all births.
Some countries have higher rates of planned homebirth. For example around 2% of all births in the UK are homebirths and in the Netherlands this is much higher at around 30%. In these countries the infrastructure for safe home birthing is well established and outcomes are usually positive.
There has been controversy about the safety of births at home with differences in opinions between health professionals and sometimes it may be difficult to obtain a balanced view.
In 2007 WA Health commissioned a review of evidence into Models of Maternity Care. This review discusses the safety of planned home births by women of low obstetric risk.
The review concluded that
"Planned home birth with a qualified home birth practitioner is a safe alternative for women determined to be at low risk of pregnancy complications." view full review-see page 11 (external site) (PDF 1.22MB)
You should be aware that your midwife will advise transfer to hospital if complications arise and that there should be a clear plan in place with your local hospital to allow a smooth transition to hospital care, should it become necessary, at any point during your pregnancy, labour or birth.
Some women opt for homebirth after a prior birth experience within a hospital environment that may have not met their expectations. For a few of these women homebirth is not a safe choice due to pre-existing medical problems or previous pregnancy or birth complications. If this applies to you we encourage you to make an appointment with senior members of midwifery and medical staff at the hospital to discuss your concerns. They will then be able to support you to ensure your next birth experience will be more rewarding.
If you are considering a homebirth make sure you are fully aware of the potential and often unpredictable complications that may arise during labour and birth before you make your choice.
Community Midwifery Program WA (external site) provides continuity of midwifery care for low-risk women who are planning to birth at home.
Royal Australian and New Zealand College of Obstetricians and Gynaecologists Homebirth statement (external site) (PDF 520KB)
Royal College of Obstetricians and Gynaecologists Homebirth statement (external site) (PDF 84KB)
Report: Review of home births in Western Australia (August 2008) (external site) (PDF 445KB)
In Australia there are a small number of women who elect to have home births. In WA, approximately 200 women have a homebirth each year representing between 0.65-0.8% of all births.
Some countries have higher rates of planned homebirth. For example around 2% of all births in the UK are homebirths and in the Netherlands this is much higher at around 30%. In these countries the infrastructure for safe home birthing is well established and outcomes are usually positive.
There has been controversy about the safety of births at home with differences in opinions between health professionals and sometimes it may be difficult to obtain a balanced view.
In 2007 WA Health commissioned a review of evidence into Models of Maternity Care. This review discusses the safety of planned home births by women of low obstetric risk.
The review concluded that
"Planned home birth with a qualified home birth practitioner is a safe alternative for women determined to be at low risk of pregnancy complications." view full review-see page 11 (external site) (PDF 1.22MB)
You should be aware that your midwife will advise transfer to hospital if complications arise and that there should be a clear plan in place with your local hospital to allow a smooth transition to hospital care, should it become necessary, at any point during your pregnancy, labour or birth.
Some women opt for homebirth after a prior birth experience within a hospital environment that may have not met their expectations. For a few of these women homebirth is not a safe choice due to pre-existing medical problems or previous pregnancy or birth complications. If this applies to you we encourage you to make an appointment with senior members of midwifery and medical staff at the hospital to discuss your concerns. They will then be able to support you to ensure your next birth experience will be more rewarding.
If you are considering a homebirth make sure you are fully aware of the potential and often unpredictable complications that may arise during labour and birth before you make your choice.
Community Midwifery Program WA (external site) provides continuity of midwifery care for low-risk women who are planning to birth at home.
Royal Australian and New Zealand College of Obstetricians and Gynaecologists Homebirth statement (external site) (PDF 520KB)
Royal College of Obstetricians and Gynaecologists Homebirth statement (external site) (PDF 84KB)
Report: Review of home births in Western Australia (August 2008) (external site) (PDF 445KB)
News from the West
From Western Australia
The following Article was published in The West Australian newspaper, Oct 13th page 17. Medical reporter Cathy O’Leary
RESPONSE [to the article below] by Community Midwifery WA
“In response to their objections we have updated the website to include a Research page – we are all for transparency and our aim is to provide women with evidence-based information to enable women to make an informed choice. See our new update page
The report was picked up by the ABC and the AMA and Simon Towler (Chief Medical Officer of WA Health) were interviewed. Dr Towler stood by their support of CMWA, the CMP and their own website “Having a Baby”.
Later on, Consumer spokesperson spoke on 6PR along with the AMA and – again – Dr Towler provide some comment. Again, the support of CMWA and CMP was very welcome.”
The following Article was published in The West Australian newspaper, Oct 13th page 17. Medical reporter Cathy O’Leary
Leading WA doctors have attacked the Health Department's promotion of home births on its website, saying it has biased information and fails to acknowledge the risks to women and their babies.
Dr Louise Farrell, the former WA head of the Royal Australian and New Zealand College of Obstetricians and Gynaecologists, and the Australian Medical Association wants the information changed or a link to the Community Midwifery Program removed .
The department's webpage on home births refers to an external website detailing advantages and disadvantages.
Last year, the department released findings of an independent review of home birth safety that found they were generally no riskier when well supported, but doctors maintain they are riskier.
Dr Farrell said the department should promote the safest and best options for women yet was publicising a practice that had poorer outcomes.
It already had to remove information promoting home birth for women who previously had a caesarean after doctors complained. "But it still seems to promote home birth as an equally safe option compared to other models and I think there's a problem with that," Dr Farrell said.
AMA WA president Dave Mountain said the department should remove the website's content until it had more balanced information.
"Choice is a good thing, but I'm against ill-informed choice and the problem with the site is that it's extremely unbalanced and portrays home birth in a way which is highly supportive and uses biased language," he said. "Although there's some research suggesting that in very well-selected people home birth can be reasonably safe, there have been significant concerns about the rates of neonatal deaths and poor outcomes."
Chief medical officer Simon Towler said the department recognised some women wanted a home birth and referred them to the CMP, a publicly-funded service for low-risk women.
He said the recent review found a planned home birth with a qualified practitioner was a safe alternative for women at low risk of complications.
But the site was being changed to include references to the review and the RANZCOG policy on home birth.
Tuesday, October 12, 2010
Monday, October 11, 2010
APMA Position Statement on Collaborative Arrangements
Australian Private Midwives Association (APMA) represents midwives in private practice.
The National Health (Collaborative arrangements for midwives) Determination 2010
As midwives become more entrenched in the medical model, midwifery skills will be lost and women's access to normal birth will be diminished even further than it is now
Private practice midwifery will become known as the model whereby midwives are working in private medical practices, with little regard for those self employed midwives who currently provide true midwifery care at this current time
Acceptance within the maternity workforce that midwives require medical sign off for Medicare and therefore further erosion of opportunity for midwives to work autonomously
The National Health (Collaborative arrangements for midwives) Determination 2010
- requires written agreement or acknowledgment by a medical practitioner for Medicare funding to be available for services provided privately by a midwife
- defies the International Confederation of Midwives (ICM) Definition of the midwife - it prevents autonomous practice for Medicare funded midwives.
- defies the ICM Declaration (Glasgow 2008) which states that legislation developed in member countries must enable midwives to practice in their own right.
- prevents most current private practice midwives from accessing Medicare funding.
- Low uptake of these reforms by midwives
- Minimal benefit to women whose seek a midwife as their primary maternity carer
- Uptake only by midwives working for obstetricians as they will be able to access the required arrangement
As midwives become more entrenched in the medical model, midwifery skills will be lost and women's access to normal birth will be diminished even further than it is now
Private practice midwifery will become known as the model whereby midwives are working in private medical practices, with little regard for those self employed midwives who currently provide true midwifery care at this current time
Acceptance within the maternity workforce that midwives require medical sign off for Medicare and therefore further erosion of opportunity for midwives to work autonomously
APMA is opposed to Parliamentary progress of the National Health (Collaborative arrangements for midwives) Determination 2010 in its current form.
APMA will continue to lobby for the National Health (Collaborative arrangements for midwives) Determination 2010 to be disallowed, withdrawn and rewritten in an acceptable form.
The NHMRC Draft National Guidance on Collaborative Maternity Care document is at http://www.nhmrc.gov.au/guidelines/consult/consultations/ngcmc.htm
Sunday, October 10, 2010
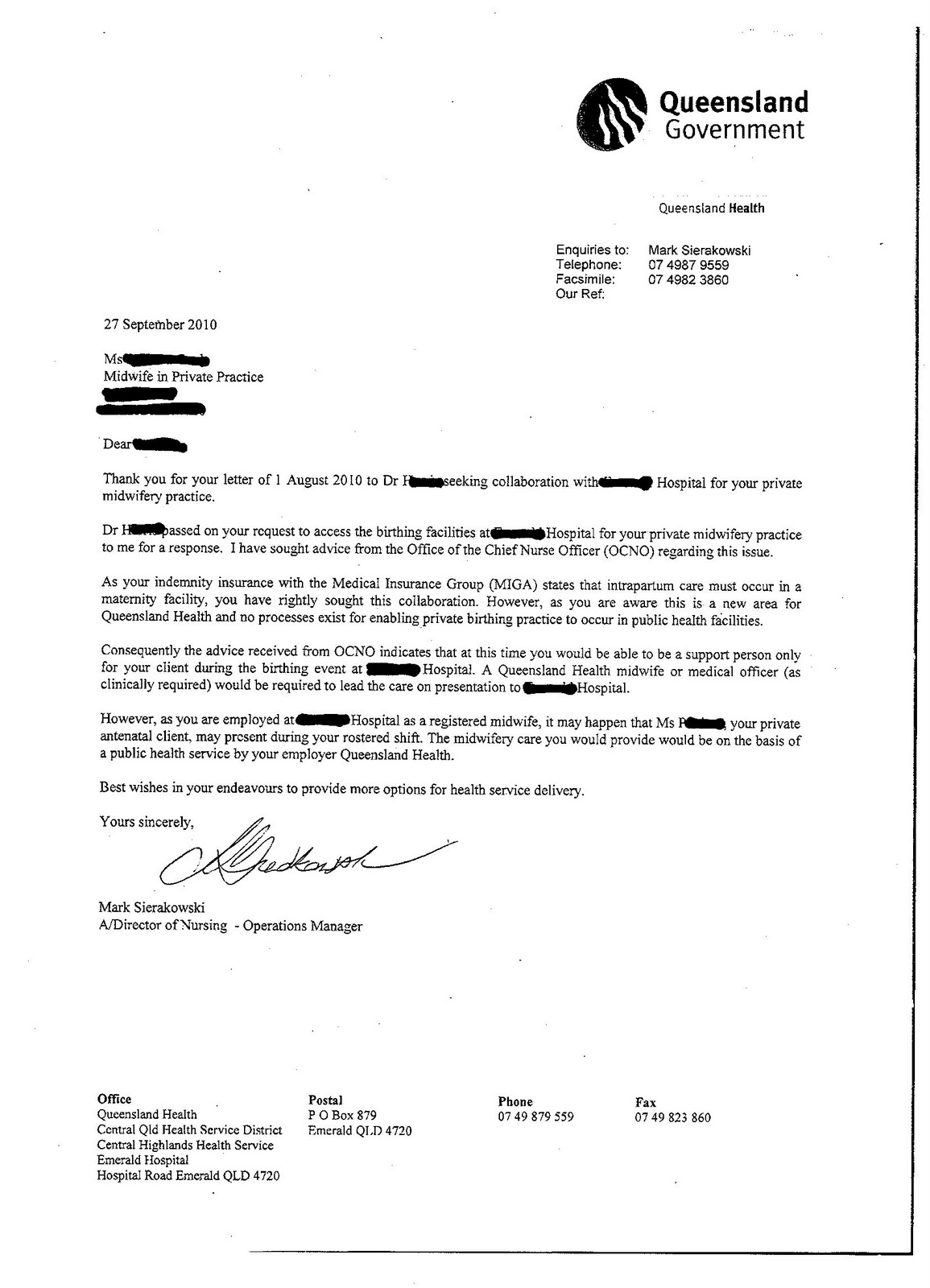
'midwifery models of care' in rural Queensland
[This account has de-identified the midwife and location. It is a clear example of the ridiculously restrictive environment in which midwives are required to practise.]
I have had various discussions with managers/project officers who are attempting to roll out hybrid 'midwifery models of care' for the rural sector. From my own personal observations -
Geographical boundaries in keeping care within local communities to ensure the care is local, owned by the consumer and feels safe (Rebirthing Report) are being ignored in the drive for efficiencies in combining some projects when viewed in a remote office in some districts.
{kind=link}
 |
| Letter |
{kind=link}
I have had various discussions with managers/project officers who are attempting to roll out hybrid 'midwifery models of care' for the rural sector. From my own personal observations -
- It is clear that GP's are the primary carer with the midwife as the after thought so as not to upset them.
- GP's are scared they will lose an income stream to their rural practice often with the right to private practice to the local hospital.
- Managers do not want to lose the doctor as the rural community backlash will be fast and vicious (rightly so).
- Higher places of office are providing non-reassuring advice to the facility managers, happy to provide details specific to my application verbally.
- It is clear managers are thinking they can switch a midwife's hat on for a few hours of the day to provide antenatal care or birth care. Essentially they are employed as a nurse first.
- It is clear until nursing workforce shortages are addressed there will be no change in practice in rural areas that ensure continuity of care with a known midwife as midwives 'offering' themselves to be in these new models are still being put on rosters and not annualised salaries plugging up nurse shortages. Burn out for midwives will occur rapidly.
Geographical boundaries in keeping care within local communities to ensure the care is local, owned by the consumer and feels safe (Rebirthing Report) are being ignored in the drive for efficiencies in combining some projects when viewed in a remote office in some districts.
Collaboration for homebirth with a General Practitioner
A well known Melbourne GP, Peter Lucas, has attended homebirths with midwives for many years.
An excerpt from his website:
Midwives are concerned that although this doctor is willing to enter what has been called a "collaborative" arrangement with a midwife, he (or his insurance company) are setting conditions on his collaboration and transferring the primary carer role from the midwife to himself. If midwives were to enter into agreements with Peter, they would no longer be the primary carer for their own clients. The arrangement negates the notion of continuity of care from the midwife who practises on her own authority, and renders useless the process of applying for Medicare/PBS eligibility for these women for their antenatal care, as the doctor will be providing that.
An excerpt from his website:
“For some 35 years Dr Peter Lucas and Wattle Park House has offered collaborative care with home birth families and the midwives they have chosen to assist them with their experiences.
"This will continue but assumes that the Wattle Park House medical practitioner attends the birth.
"Until midwives obtain full indemnity cover which includes the labour and delivery, collaboration at a distance is fraught with uncertainty in a medico-legal sense, and cannot be seriously entertained.”
Midwives are concerned that although this doctor is willing to enter what has been called a "collaborative" arrangement with a midwife, he (or his insurance company) are setting conditions on his collaboration and transferring the primary carer role from the midwife to himself. If midwives were to enter into agreements with Peter, they would no longer be the primary carer for their own clients. The arrangement negates the notion of continuity of care from the midwife who practises on her own authority, and renders useless the process of applying for Medicare/PBS eligibility for these women for their antenatal care, as the doctor will be providing that.
Saturday, October 9, 2010
Examples of lack of collegiality by some doctors
In preparation for the implementation of Medicare reforms, commencing 1 November, midwives and maternity consumers have been asked to record evidence of any obstruction to collaboration.
The following message has been received from a midwife in Melbourne:
NOTE:
The Australian Medical Association has published a document Collaborative Arrangements: What you need to know in preparation for the inclusion of eligible midwives and nurse practitioners in Medicare funding from 1 November 2010.
This guide is intended to provide you with guidance on important information to consider when entering into a collaborative arrangement with a midwife or nurse practitioner.
Contents:
Link to Medicare information: Midwives and Nurse Practitioners
The following message has been received from a midwife in Melbourne:
"A number of my clients have been advised by the GP, when going to their office requesting blood tests, ultrasounds etc, that if they are having a midwife attended home-birth then the GP does not want to be involved in their care beacuse of the lack of insurance for midwives in private practice. This is a major barrier to collaboration in my opinion. I have been searching RACGP websites for some confirmation of this issue and have found some. The attached document (the RACGP submission to government) states:
"What are the workforce barriers to integrated models of care?
• Insurance
As stated previously the RACGP finds the present unavailable of insurance for
privately employed midwives a deterrent. Some GPs want to access midwives on a
sessional basis as they do for other doctors, but find this not possible in the current
climate."
Link:
"Do any of the Midwives/clients have it in writing that GP's are refusing to collaborate already? I have personally found this to be a frustrating and potentially negilgent treatment of women. They [the women] ask for a simple test and the GP refuses - what if there IS an undetected problem because of the GP's refusal to provide care?"
NOTE:
The Australian Medical Association has published a document Collaborative Arrangements: What you need to know in preparation for the inclusion of eligible midwives and nurse practitioners in Medicare funding from 1 November 2010.
This guide is intended to provide you with guidance on important information to consider when entering into a collaborative arrangement with a midwife or nurse practitioner.
Contents:
- The legislation
- Effective collaboration is good for patients
- What is a collaborative arrangement?
- Does the midwife/nurse practitioner meet the relevant MBS/PBS requirements?
- Indemnity insurance
- Is there any obligation to participate in a collaborative arrangement?
- Are there any restrictions on which medical practitioners can participate in a collaborative arrangement?
- Can more than one medical practitioner be a party to a collaborative arrangement?
- Is a collaborative arrangement required for every patient?
- Do you have confidence in the midwife or nurse practitioner?
- Remuneration
- Should you insist on a written agreement?
- Clinical settings where services will be provided
- What matters should be included in a collaborative arrangement?
- Best practice guidelines
- What should you do when a patient does not want to follow agreed clinical guidelines?
- What happens if things do not work out?
- Where can you obtain more information about relevant MBS and PBS arrangements?
Link to Medicare information: Midwives and Nurse Practitioners
New blogger
 |
| That's me at a rally outside the Health Minister's office |
{kind=link}
I would like to introduce myself, as I have put my hand up to work with this blog. My blogs are perhaps the best way of telling you how I use this valuable medium.
Through the villagemidwife blog I share my own midwifery stories and make critical comment on current issues.
midwivesVictoria is a site I manage for the Midwives in Private Practice (MiPP) group, a collective of independent midwives in Victoria.
Private Midwifery Services is a more recent blog, in which I have addressed the very complex and often vexed issue of reform of maternity services, particularly as it has impacted on independent practice including homebirth.
My blogging experience goes back several years. On my blogger dashboard I have about a dozen sites, and there's a Word Prss quilt blog out there too! I use blogs as records that are maintained in a systematic fashion over time, and easily retrieved. A blog is like a magazine that, instead of having pages that you turn, has pages that continue on down the screen and into the past. The links on the side bar of the blog invite the reader to explore further. Documents and posters can be posted on the blog as images, and enlarged by a right click from the mouse.
Anyone who is older than about 40 will remember the pre-digital, pre-internet era. As a budding activist for maternity reform as recently as the early 1990s, I did cutting and pasting of articles that were put together into a photocopied magazine, or a single page. We had a computer and a printer, but there was no ability to do special page layouts. Instead of mail merge for addresses, we addressed envelopes by hand. The marvel of fax could be used then to get messages out quickly to hospital maternity units.
Then came email, firstly through the Uni, and then at home. What emancipation!
The world of midwifery, and maternity activism, has groups that connect with each other through direct email, Yahoo! groups, and in recent years other social networks such as Facebook and Twitter. In those groups it's very easy to become inwardly focused, with pretty well everyone speaking the same language, or at least those who engage in discussion are. And there is usually, in my experience, a silent majority.
A blog enables information to be shared with anyone who is interested. The networks formed by blogs, with links to other similar blogs and websites, can lead readers down interesting and complex pathways. This crossing of professional and cultural boundaries is useful as an adjunct to the more restricted group discussions.
Blogs enable tracking of numbers of visitors to the site: a sort of statistical self-worth meter. Comments are useful, sometimes agreeing, and sometimes putting an opposing view. The hardest thing for a blogger to face is the doldrums, when noone out there seems interested in all the fascinating material that one has collected and shared. Photos can be used too, and will often draw attention to an otherwise bland page of text.
Australian Private Midwives Association welcomes our readers. Comments that address issues of interest to our group are welcome.
Subscribe to:
Posts (Atom)